
Also available in: Español
By Joan Tallada
(This note was taken from the Social Dialogues methodology, that was tested in a pilot project implemented in Paraguay, Panama and Belize during the period between November 2016 and February 2017, in the framework of the studies promoted by the LAC Platform)
Why a proposal to support the sustainability of civil society?
The dawning of a new period that evolves towards self-sustenance with national resources in a number of countries receiving support from the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM), together with the implementation of the corresponding GF’s transition, sustainability and co-financing policy, has driven the proliferation of proposals and facilitation tools as of lately.
Among other tools are included the “Transition Preparedness Assessment Framework Tool” developed by Curatio International Foundation, the “Social Contracting Tool” by APM Global Health, and “Transition Readiness Assessment Tool” by Eurasian Harm Reduction Network with the collaboration of AMPG Health, which have already begun to be applied in several places.
Such instruments are certainly useful because, one way or another, they help to better understand the gaps and opportunities to sustain the response within the scope of current HIV/AIDS, Tuberculosis and Malaria relations. However, its application may be limited or even halted if civil society is not duly prepared with a process of cultural and organizational transition that provides the understanding on how the expectations of general society are changing with regards to the use of domestic resources, in which ways the latter redefines the rules of the national political game, and how all this forces civil society to rethink and reposition itself as key players in the sustainable responses.
In other words, it is necessary, albeit not sufficient, to equip civil society with technical instruments for the demand and management of services in HIV, Tuberculosis and Malaria. Previous or simultaneously, it is also necessary to increase their capacity for analysis and action on how to sustain the social legitimacy of such services and how to ensure a timely political and budgetary response that complies therewith.
The whole society is in transition
The Latin America and the Caribbean (LAC) region, just like the rest of the planet in varying degrees, is undergoing fundamental changes in several areas that will determine the setting, opportunities and challenges for an effective response to HIV, TB and Malaria. These changes require civil society to undergo a process of reflection and critical adaptation into a new framework of relations with general society and with those who design, approve, implement and evaluate public policies in their countries for health or other related sectors. This document and the methodological process proposed hereby are aimed at supporting and stimulating civil society in the LAC region in order to encourage taking an active role and making a significant contribution to ensure that those changes fully integrate the effective response to the three diseases abovementioned.
The term most commonly used to designate transformations in progress is “transition”, which may be ambiguous, since it designates an intermediate step between two conditions, a previous one and a subsequent one, which is intended to be well defined, but that not always fits reality. However, its use has become widespread in academic and official documents as well as in international meetings, and it is therefore used in this document. Its application to specific countries must be done with the due precautions and nuances.
Four interlinked transitions are changing the health landscape in LAC: The transition of funding sources for HIV, TB and Malaria programs (among others), the transition from international commitments to health, the transition of diseases or epidemiological transition, and the population or demographic transition.
Subsequently, we will explain briefly each of the abovementioned transitions, commenting on the implications for the region and for civil society action and sustainability strategies for HIV, TB and Malaria. This exhibition aims to provide analysis tools of a changing environment wherein community groups must conduct, analysis that argument the subsequent proposals for action.
In a second part, we propose the basis of a methodology for critical reflection on the environment and the definition of an action plan, including the identification of support and training needs which will facilitate civil societies of HIV, TB and malaria to meet the challenges and take advantage of the opportunities offered by these new scenarios as they become evident in their respective countries. This methodology was tested in a pilot project implemented in Paraguay, Panama and Belize during the period between November 2016 and February 2017. The implementation experiences in these three countries have been used to evaluate and improve the methodology. The results of these processes can be obtained through the following links:
- Transitioning and sustainability of civil society in the HIV/TB response of Belize
- Report on Technical Assistance Risks and Needs of Civil Society in the Context of Sustainable Transition in Panama
- Sustainability of Community Response Actions to HIV, TB and Malaria in Paraguay
Latin America and the Caribbean in Transition
Transition of funding sources for HIV, TB and Malaria programs
Although the economic data for the past two years are negative, if taken from a three decades perspective Latin America and Caribbean countries have been gradually increasing their average income per capita [1]. While this indicator does not reflect how equitably the income is distributed among the population sectors, the average value is adequate to progressively cease to being considered eligible to receive total or partial aid from entities such as GAVI (the Vaccine Alliance) or The Global Fund to Fight AIDS, Tuberculosis and Malaria, or other bilateral agencies from high-income countries.
The expectation of the international community is that the governments of countries that until now were recipients are now able to raise more revenues from taxes from an upward economic activity and to use it to provide better basic social services, for example, education and health. The source of such taxes is often an emerging middle class that is increasingly connected, more involved and more demanding towards their governments.
Thus, the countries of the LAC region are increasingly dedicating more of their own funds to their own health systems, while donor countries are contributing less. This combined phenomenon also implies a change of legitimacies: While international agencies respond to boards of directors that include representatives of multiple actors, national leaders must be accountable to their own complex, unequal and hierarchical societies, where the preservation of the human rights of minorities does not necessarily have the adequate support.
This raises the need for the civil society of HIV, TB and Malaria to reconsider its strategy, which until now has often been focused -regarding the financial sustainability of the response of civil society- in the relationship with bilateral or multilateral donors, shifting towards the dialogue and the advocacy in the field of local public institutions and in the society as a whole to which they are accountable to.
The transition of international commitments in health
In 2000, the United Nations General Assembly unanimously approved the so-called Millennium Development Goals (MDGs), an international commitment that resulted in an unprecedented transfer of resources from high-income countries to low and middle-income countries. Out of the 8 goals, 3 were related to health, and one in particular, namely number 6, was focused on the fight against HIV, malaria, and other diseases, such as tuberculosis. The commitments related to these MDGs formally expired in 2015.
In September of 2015, the 193 countries that make up the same General Assembly of the United Nations, among which are those from Latin America and the Caribbean, adopted the so-called Agenda 2030 and the commitment to adhere to the Sustainable Development Goals (SDGs). These are 17 goals, of which number 3 refers directly to health: “Ensure healthy lives and promote well-being for all at all ages.” A guarantee that is the responsibility of all governments, regardless of their level of wealth.
Thus, the international agenda to which the countries of the LAC region have adhered transits from a perspective focused on the reduction of mortality associated with specific diseases or populations (the so-called vertical approach) to another one, that although it still mentions them[2], puts greater emphasis on improving the general health of all people (the so-called horizontal approach).
This generalization of the international health agenda requires changing the discussion of the actors that until now have been involved in its implementation, including civil society, as it modifies both the number as well the interests and the framework of their relationship.
The transition of diseases or epidemiological transition
In the past 25 years, the profile of the diseases with greater weight[3] among the general population for the whole of the LAC region has been varying: whereas in 1990, communicable diseases and maternal and child diseases were most prevalent, nowadays their place has been taken by non-communicable diseases, although closely followed by firearm assaults and the persistence of lower respiratory tract infections[4].
Scenarios may vary when analyzing the situation in each country, each population group and each disease. In the case of HIV, the burden of disease compared to the set of health problems that cause death and disability is very high in Belize[5] and Dominican Republic, and significant in Panama, whereas, compared to the rest of ailments, it is not the case in Ecuador, Peru or Paraguay, where it does not appear in the list of the top 20 diseases with greater burden. As for tuberculosis or malaria, neither of them is listed in any of the countries mentioned.
Although the analysis varies and gives greater weight to the three diseases if specific groups are taken, such as the indigenous population or the reproductive age (15-49), and mortality is used as an indicator, we must remember that health policies and systems are shifting their focus towards increasing health gains for the general population rather than to reducing deaths in specific groups. The fact that this generates questions of inequity does not prevent it from being taken into account when determining the viability of action strategies.
Changes in the epidemiological profile of the region as a whole, and the way in which they reproduce or not in each sub region, country, or population group, have important consequences on where the focus of public health policy stands and the expectations that general society has about them.
Where the data shows a persistence or an increase in the burden of disease, as is the case of HIV in Central America and the Caribbean, the civil society’s strategy must be different from that of the other nations, such as in South America, where these particular diseases have a much lower weight, and the demands of the general society about which should be public priorities for health intervention do not necessarily take them into account.
In addition, in the case of HIV, the evolution experienced by its approach should be taken into account given the expansion of the antiretroviral treatment coverage, the effect of such treatment on the transmission risk and the potential use of pre-exposure prophylaxis. In this regard, the emphasis shifts towards ensuring early detection and the treatment cascade rather than reinforcing behavior change programs or policies for modifying risk determinants among vulnerable populations.
Population or demographic transition
Parallel to the transition of diseases, LAC is experiencing the transition of populations, also called demographic transition: in 1990, the younger age groups had a much higher weight in the population as a whole, while in 2016 this weight is distributed more evenly, a trend that is accentuated in the projections for the coming years
(see Figure 1).
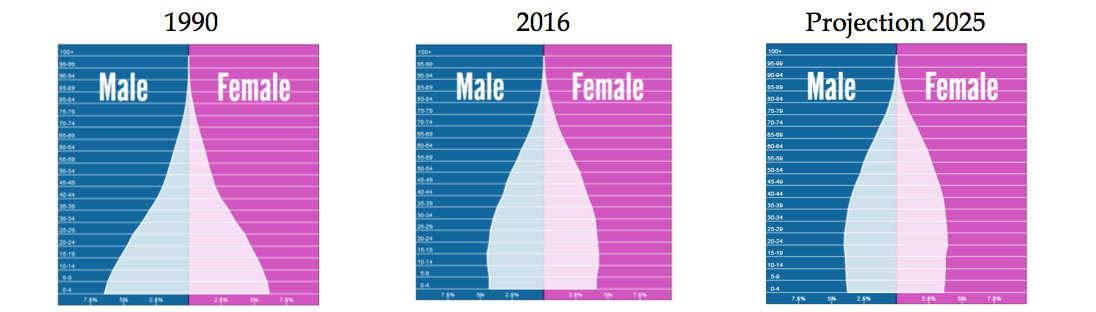
Figure 1: Population pyramid in Latin America and the Caribbean expressed by age and gender groups in 1990, 2016 and the forecast for 2025. Source: www.populationpyramid.net
These projections point to an increase in life expectancy and the consequent aging of the population, which runs parallel to the increase in non-communicable diseases observed in the previous section.
It is true that, as it has been discussed, the impact of the three diseases by age group, the burden of HIV or tuberculosis among people of reproductive age (15-49 years) moves up several positions in some countries; but it is also true that the demographic composition will condition social expectations regarding the priorities that health systems must set forth.
Identifying the Challenges of Civil Society in Transition
The transitions described in the previous section compel civil society to exercise reflection and analysis about what are the big changes taking place in their environment and how they stand and act thereon.
This exercise is further driven by the Global Fund’s transition, sustainability and co-financing policy to Fight AIDS, TB and Malaria, which supports sustainable transition processes, including the preparation of civil society and communities to participate in such processes through collective reflection, the identification of needs and the planning of the corresponding actions.
Objectives
The following sections offer a number of tools that civil society groups on HIV, tuberculosis and malaria in each country can use to achieve these two goals:
- Building a shared vision on changes in the social, political, and financial environment and the challenges and opportunities that this entails for civil society in HIV, TB and malaria.
- Develop an action plan that lays the foundations for addressing the challenges and take advantage of the opportunities presented by the transition processes. This action plan should detail the training and support needed to carry it out.
Methodology
This process shall be conducted following a participatory methodology using the analysis and interpretation of the available evidence, the opinion of experts and key players, and dialogue and agreement among peers.
Final products
At the end of this process in each of the countries where it is applied, the following products shall be available:
- The shared vision of civil society groups on how the transition is developing in their country, what the challenges and opportunities are.
- A plan with proposals for action, responsible people and institutions, and the corresponding implementation schedule. Said plan will have a section that defines the support and training necessary for its implementation and shall be accompanied by a corresponding budget prepared with the help of local consultants.
[1] “América Latina y el Caribe: panorama general”. The World Bank: http://www.worldbank.org/en/region/lac/overview (accessed on 11/16/2016).
[2] Of the 13 targets of the said goal number 3, the third one is committed to “put an end to AIDS, tuberculosis, malaria epidemics and neglected tropical diseases, and fight hepatitis, waterborne diseases And other communicable diseases by 2030”
[3] The burden of disease is expressed in “Disability Adjusted Life Years” or DALYs, which expresses the years lost due to premature death and the reduction of optimal quality of life as a result of a health problem. There is agreement among experts that all public health policy should aim at reducing the burden of DALYs in the population.
[4] Burden of disease expressed in DALYs in Latin America and the Caribbean for 1990 and 2015. Source: vizhub.healthdata.org/gbd-compare
[5] It has gone from being the first to the second disease, behind diabetes, in DALYs for the population as a whole, although it continues to be first in both DALY and premature mortality for adults between 18 and 49 years of age. Source: vizhub.healthdata.org/gbd-compare